Dupuytren's contracture
Introduction
Dupuytren's contracture is a fairly common disorder of the fingers. It most often affects the ring or little finger, sometimes both, and often in both hands. Although the exact cause is unknown, it occurs most often in middle-aged, white men and is genetic in nature, meaning it runs in families. This condition is seven times more common in men than women. It is more common in men of Scandinavian, Irish, or Eastern European ancestry. Interestingly, the spread of the disease seems to follow the same pattern as the spread of Viking culture in ancient times. The disorder may occur suddenly but more commonly progresses slowly over a period of years. The disease usually doesn't cause symptoms until after the age of 40.
This guide will help you understand how Dupuytren's contracture develops how the disorder progresses, and how you can measure its progression what treatments are available
Anatomy
What part of the hand is affected?
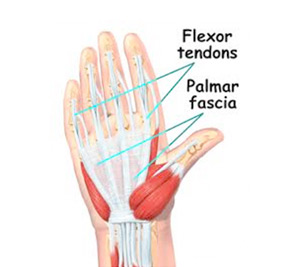
The palm side of the hand contains many nerves, tendons, muscles, ligaments, and bones. This combination allows us to move the hand in many ways. The bones give our hand structure and form joints. Bones are attached to bones by ligaments. Muscles allow us to bend and straighten our joints. Muscles are attached to bones by tendons. Nerves stimulate the muscles to bend and straighten. Blood vessels carry needed oxygen, nutrients, and fuel to the muscles to allow them to work normally and heal when injured. Tendons and ligaments are connective tissue.
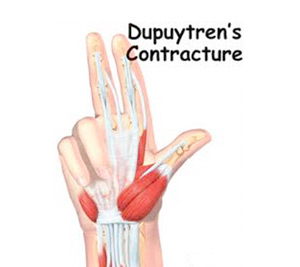
Another type of connective tissue, called fascia, surrounds and separates the tendons and muscles of the hand. Lying just under the palm is the palmar fascia, a thin sheet of connective tissue shaped somewhat like a triangle. This fascia covers the tendons of the palm of the hand and holds them in place. It also prevents the fingers from bending too far backward when pressure is placed against them. The fascia separates into thin bands of tissue at the fingers. These bands continue into the fingers where they wrap around the joints and bones. Dupuytren's contracture forms when the palmar fascia tightens, causing the fingers to bend.
The condition commonly first shows up as a thick nodule (knob) or a short cord in the palm of the hand, just below the ring finger. More nodules form, and the tissues thicken and shorten until the finger cannot be fully straightened. Dupuytren's contracture usually affects only the ring and little finger. The contracture spreads to the joints of the finger, which can become permanently immobilized.
Causes
Why do I have this problem?
No one knows exactly what causes Dupuytren's contracture. The condition is rare in young people but becomes more common with age. When it appears at an early age, it usually progresses rapidly and is often very severe. The condition tends to progress more quickly in men than in women.
People who smoke have a greater risk of having Dupuytren's contracture. Heavy smokers who abuse alcohol are even more at risk. Recently, scientists have found a connection with the disease among people who have diabetes. It has not been determined whether or not work tasks can put a person at risk or speed the progression of the disease.
Symptoms
What does Dupuytren's contracture feel like?
Normally, we are able to control when we bend our fingers and how much. How much we flex our fingers determines how small an object we can hold and how tightly we can hold it. People lose this control as the disorder develops and the palmar fascia contracts, or tightens. This contracture is like extra scar tissue just under the skin. As the disorder progresses, the bending of the finger becomes more and more severe, which limits the motion of the finger.
Without treatment, the contracture can become so severe that you cannot straighten your finger, and eventually you may not be able to use your hand effectively. Because our fingers are slightly bent when our hand is relaxed, many people put up with the contracture for a long time. Patients with this condition usually seek medical advice for cosmetic reasons or the loss of use of their hand. At times, the nodules can be very painful. For this reason many patients are worried that something serious is wrong with their hand.
Diagnosis
How do doctors identify the problem?
Your doctor will ask you the history of your problem, such as how long you have had it, whether you've noticed it getting worse, and whether it has kept you from doing your daily activities. The doctor will then examine your hand and finger.
Your doctor can tell if you have a Dupuytren's contracture by looking at and feeling the palm of your hand and your fingers. Usually, special tests are unnecessary. Abnormal fascia will feel thick. Cords and small nodules in the fascia may be felt as small knots or thick bands under the skin. These nodules usually form first in the palm of the hand. As the disorder progresses, nodules form along the finger. These nodules can be felt through the skin, and you may have felt them yourself. Depending on the stage of the disorder, your finger may have started to contract, or bend.
The amount you are able to bend your finger is called flexion. The amount you are able to straighten the finger is called extension. Both are measured in degrees. Normally, the fingers will straighten out completely. This is considered zero degrees of flexion (no contracture). As the contracture causes your finger to bend more and more, you will lose the ability to completely straighten out the affected finger. How much of the ability to straighten out your finger you have lost is also measured in degrees.
Measurements taken at later follow-up visits will tell how well treatments are working or how fast the disorder is progressing. The progression of the disorder is unpredictable. Some patients have no problems for years, and then suddenly nodules will begin to grow and their finger will begin to contract.
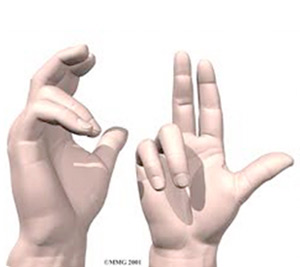
The tabletop test may also done. The tabletop test will show if you can flatten your palm and fingers on a flat surface. You can follow the progression of the disorder by doing the tabletop test yourself. Your doctor will tell you what to look for and when you should return for a follow-up visit.
Treatment
What can be done for the condition?
There are two types of treatment for Dupuytren's contracture: surgical and nonsurgical. The best course of treatment is determined by how far the contractures have advanced.
Nonsurgical Treatment
In the early stages of this disorder, frequent examination and follow-up is recommended. Your doctor may inject cortisone into the painful nodules. Cortisone can be effective at temporarily easing pain and inflammation. Heat and stretching treatments given by a physical or occupational therapist may also be prescribed to control pain and to try to slow the progression of the contracture.
Treatment also consists of wearing a splint that keeps the finger straight. This splint is usually worn at night.
The nodules of Dupuytren's contracture are almost always limited to the hand. If you receive regular examinations and follow your doctor's advice, you may be able to slow the problems caused by this disorder. However, Dupuytren's contracture is known to progress, so surgery may be needed at some point to release the contracture and to prevent disability in your hand.
Surgery

No hard and fast rule exists as to when surgery is needed. Surgery is usually recommended when the joint at the knuckle of the finger reaches 30 degrees of flexion. When patients have severe problems and require surgery at a younger age, the problem often comes back later in life. When the problem comes back or causes severe contractures, surgeons may decide to fuse the individual finger joints together. In the worst case, amputation of the finger may be needed if the contracture restricts the nerves or blood supply to the finger.
Surgery for the main knuckle of the finger (at the base of the finger) has better long-term results than when the middle finger joint is tight. Tightness is more likely to return after surgery for the middle joint.
Tissue Release
The goal of tissue release surgery is to release the fibrous attachments between the palmar fascia and the tissues around it, thereby releasing the contracture. Once released, finger movement should be restored to normal. If the problem is not severe, it may be possible to free the contracture simply by cutting the cord under the skin. If the palmar fascia is more involved and more than one finger is bent, your surgeon may take out the whole sheet of fascia.
Palmar Fascia Removal
Removal of the entire palmar fascia will usually give a very good result. The cure is often permanent but depends a great deal on the success of doing the physical or occupational therapy as prescribed. Little ill effect is caused by removing the entire palmar fascia, although the fingers may bend backward slightly more than normal. If you decide to have this surgery, you must commit to doing the therapy needed to make your surgery as successful as possible.
Skin Graft Method
A skin graft may be needed if the skin surface has contracted so much that the finger cannot relax as it should and the palm cannot be stretched out flat. Surgeons graft skin from the wrist, elbow, or groin. The skin is grafted into the area near the incision to give the finger extra mobility for movement.
Rehabilitation
What should I expect after treatment?
Nonsurgical Rehabilitation
The ability of nonsurgical treatments to slow or actually reverse the contracture is not all that promising. The contracture usually requires surgery at some point. Heat, stretching, and a finger splint seem to help the most. These treatments may be directed by a physical or occupational therapist. Sessions may be scheduled for a few visits per week up for up to six weeks, but after that, you'll probably be instructed to continue using the splint and doing the stretches as part of a home program for several months.
After Surgery
Your hand will be bandaged with a well-padded dressing and a splint for support after surgery. Physical or occupational therapy sessions may be needed after surgery for up to six weeks. Visits will include heat treatments, soft tissue massage, and vigorous stretching. Therapy treatments after surgery can make the difference in a successful result after surgery.